Focuses on improving the appearance of teeth, gums, and smile. Includes procedures like whitening, veneers, bonding, and contouring. Often uses advanced materials for natural-looking results. May also have functional benefits. Increasingly popular due to demand for a better smile.

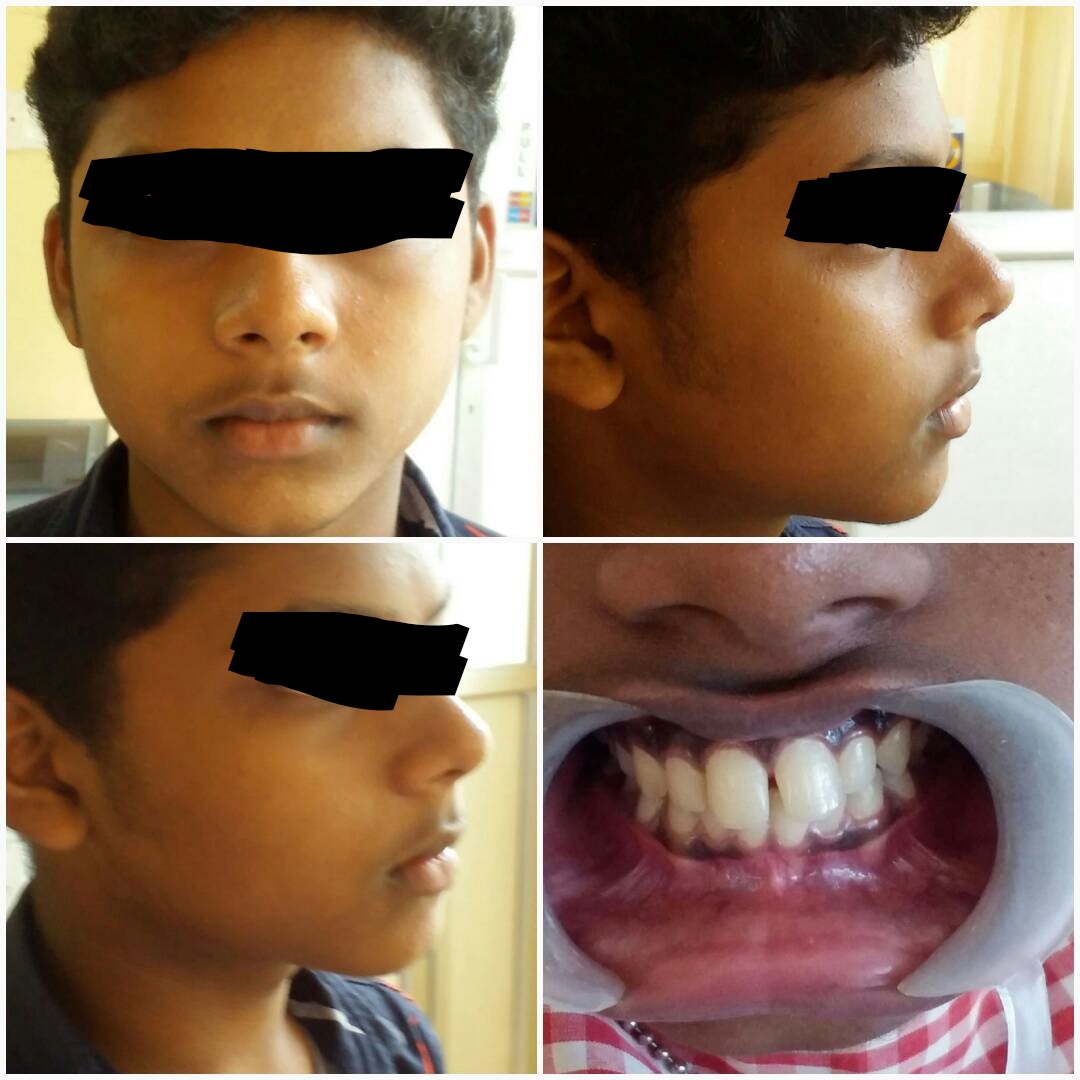
Before: The individual needed correction of a discoloured tooth and closure of spacing between teeth.

After: The individual needed correction of a discoloured tooth and closure of spacing between teeth.
Space between central incisor was corrected using tooth colored filling material

Before:

After:
Discolored central incisor was corrected using tooth colored filling material

Before:

After:
Fractured Tooth

Fractrured tooth needed management

Correction of fractured tooth with tooth coloured filling material
Fractured Tooth Management with Root Canal

Fractrured tooth needed management

After root canal treatment and post palcement

Correction of fractured tooth with tooth coloured filling material.

Xray of tooth after Root canal treatment and popst palcement.
Veneers
Improvements in materials and techniques for adhesive Dentistry, has given the restorative Dentist the option for treatment which are more conservative and aesthetic than before. One of the important developments is Cosmetic dentistry in the last of twentieth century was the development of dental Veneers especially ceramic veneers. Veneers can be made by using Dental composite (tooth coloured filling material) which can made directly on the tooth or indirectly where it is fabricated outside on models as ceramic veneers, and placed on to the tooth using a bonding agent and resin glue The disadvantage of composite dental veneers is that, they get easily dislodged when involving the incisal tip of the tooth but of the dental veneers are kept away from the insisal tip of the tooth, their chances of success is high and the added advantage of composite dental veneer is that they can be repaired easily by the application of dental composites.Ceramic veneers
They are made from a shell of tooth, (ceramic) which covers the labial as well as the incisal area (insiso They are -lingual ) like a butt joint. The advantage of dental ceramic veneers is that less tooth reduction is needed compared to a dental crown. Much stronger than a dental composite veneers, which can fracture easily, but if the dental ceramic veneer is subjected to excessive clenching or compression forces it can fracture or cleaves away from the tooth. Though there are advantages and disadvantages of dental ceramic and dental composite veneers depending on the aesthetic needs, area of tooth which needs replacement or correction dental composites or dental ceramics can be the material of choice of the treatment for dental veneers.Metal free ceramic crowns
Metal free ceramic crowns one of the most aesthetic dental crowns in the market, where instead of a metal substructure, a ceramic batching is used as the base of ceramic, it has the advantage that it doesn’t from a black line along the gum margin, due to the corrosion of metal backing along the cervical margins of the metal ceramic crowns. But metal free ceramic crowns has the disadvantage that they fracture easily when masticatory forceses are exerted on them. Provided gum recessions, which can form due to age, improper maintenance of oral care along the gum margins of the dental crowns are also seen in metal free ceramic crowns also. Metal ceramic crowns Ceramic fused to metal has the strength of metal and aesthetics of ceramics ceramic fused to metal restorations has an initial coping which fits over the stump, over which ceramic is added. The metal coping will be a thin layer at the gingival margin, and certain times a small part of the metal is removed and instead ceramic is added over that area. Metal ceramic crown has three layers, an opaque porcelain to mask the opaque colour of metal body porcelain and incisal porcelain. One of the major reasons for acceptance of ceramic fused to metal crown, was due to the strength of metal and its ability to bond to the ceramic metal. But one of the major disadvantages of metal ceramic crown was the formation of a black line along the cervical margin due to the exposure of the metal to oral fluids and formation of corrosion products this affecting the aesthetic appearance of the crown.Addresses the dental needs of older adults. Manages issues like dry mouth, tooth loss, and gum disease. Emphasizes prevention and coordination with medical care. Promotes comfort and oral function in elderly patients. Supports improved quality of life for aging populations.
Dry mouth can be avoided by
- Using oral moisturizers, such as mouth wash.
- Drinking plenty of water, even if not thirsty
- Using sugar free gums to stimulate salivation production.
- Avoid food and beverages which can cause irritation to oral mucosal tissues.
- Consult a Dentist and get fluoride varnish to protect the teeth from cavities.
Many older adults have gum and periodontal problems which is due to plaque which irritate the gums and make then swollen, red and which makes them bleed.
One difficulty of gum problem is that it is a painless condition until to the advanced stage. If they are left untreated the gums detach from the teeth and leads to plaque and food accumulation and eventually damage to the supporting structures of the tooth and loss of tooth itself.
Prevention of gum problems
Prevention of calculus by proper brushing technique using interdental brushes, and oral irrigators which helps to flush out lodged food debris between tooth and thus prevent gum inflammation.
Root caries
Another common problem see is root caries, which is caused by lodgement of food inter-proximally and which if not removed will end up in root caries.
Advantage or retaining natural tooth
The function of your smile will be much better with natural tooth, than artificial (prosthetic) tooth. Even through dental bridges and implants can give a good appearance some thing that is natural cannot be replaced by artificial means. Provided there is no difficulty as such of removable dentures, which has to cleaned for removal and even kept out of the oval cavity during night. Retention of natural teeth is cheap in the long run. A mouth without tooth is like a mill without a blades natural tooth are precious and should be lead to preserved at any cost, by the various treatment modalities which are available for us in the Dental fraternity.
Specializes in restoring and replacing missing or damaged teeth. Involves crowns, bridges, dentures, and implants. Aims to restore function, aesthetics, and oral health. Handles complex reconstructive cases. Often works with other dental specialists for full-mouth rehabilitation.

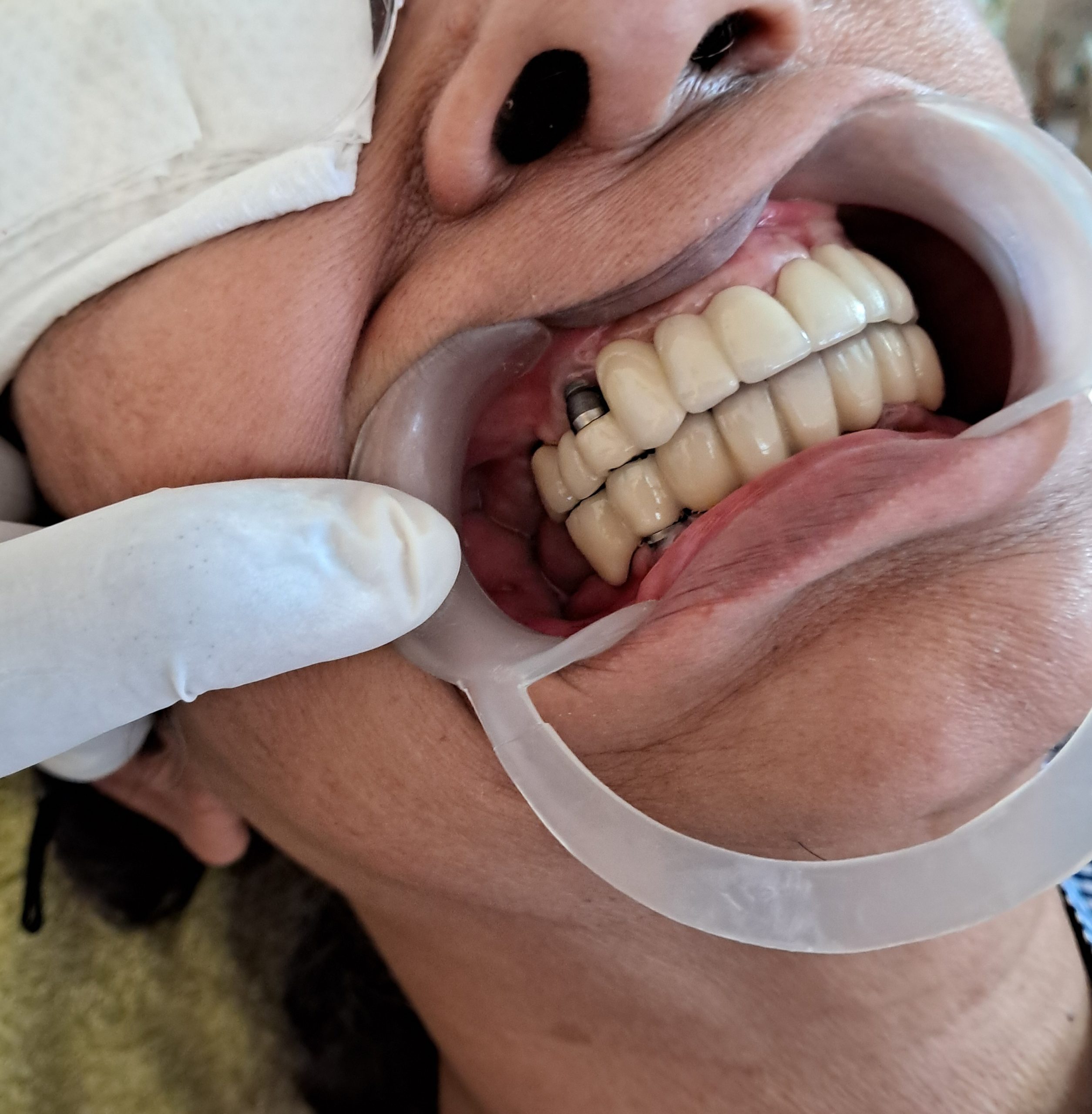
Before:Needed replacemrnt of toothin upperjaw and lower missing tooth

After: Tooth repalceemnt in upper and lower jaw
Deals with diseases of the dental pulp and root tissues. Main procedure is root canal treatment. Saves infected teeth and relieves pain. Uses advanced tools and techniques for precise care. Prevents tooth loss and maintains oral health.
Root Canal
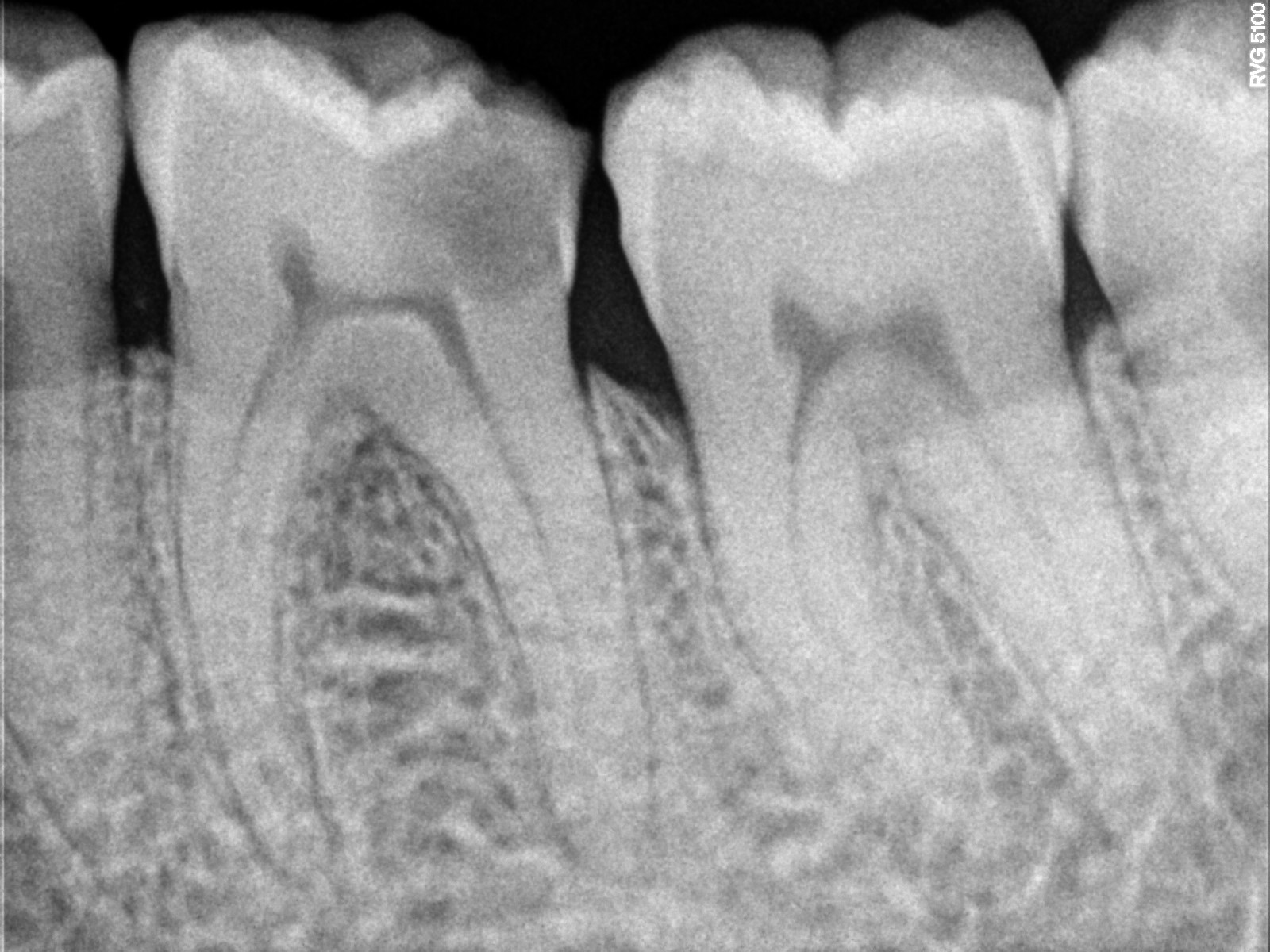
Before: Lower jaw teeth needed Root Canal treatment, due to pain.
After: Tooth after Root Canal treatment.

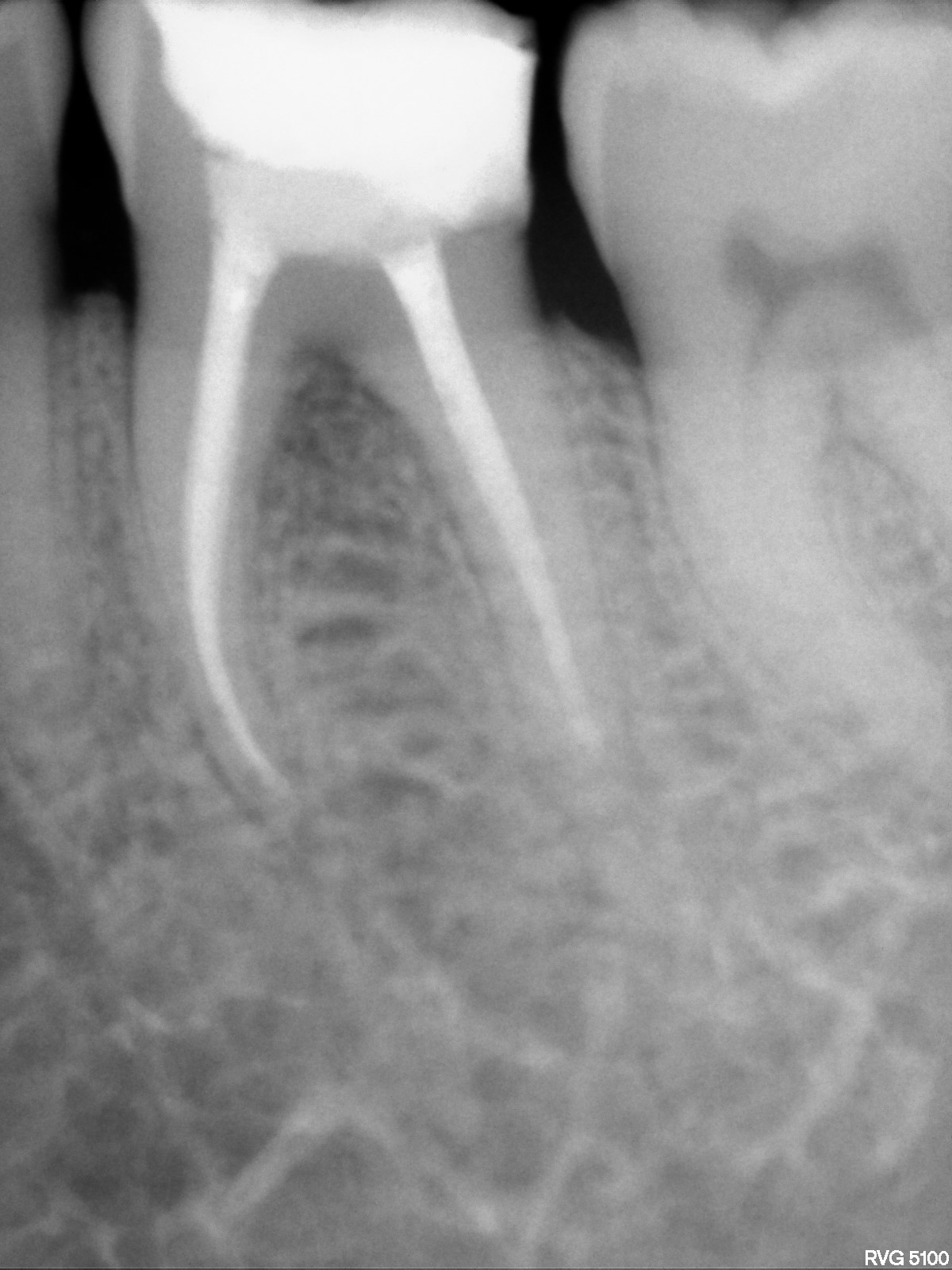
Before: Lower teeth needed Root canal treatment, due to history of pain.

After:Lower teeth after Root Canal Treatment.
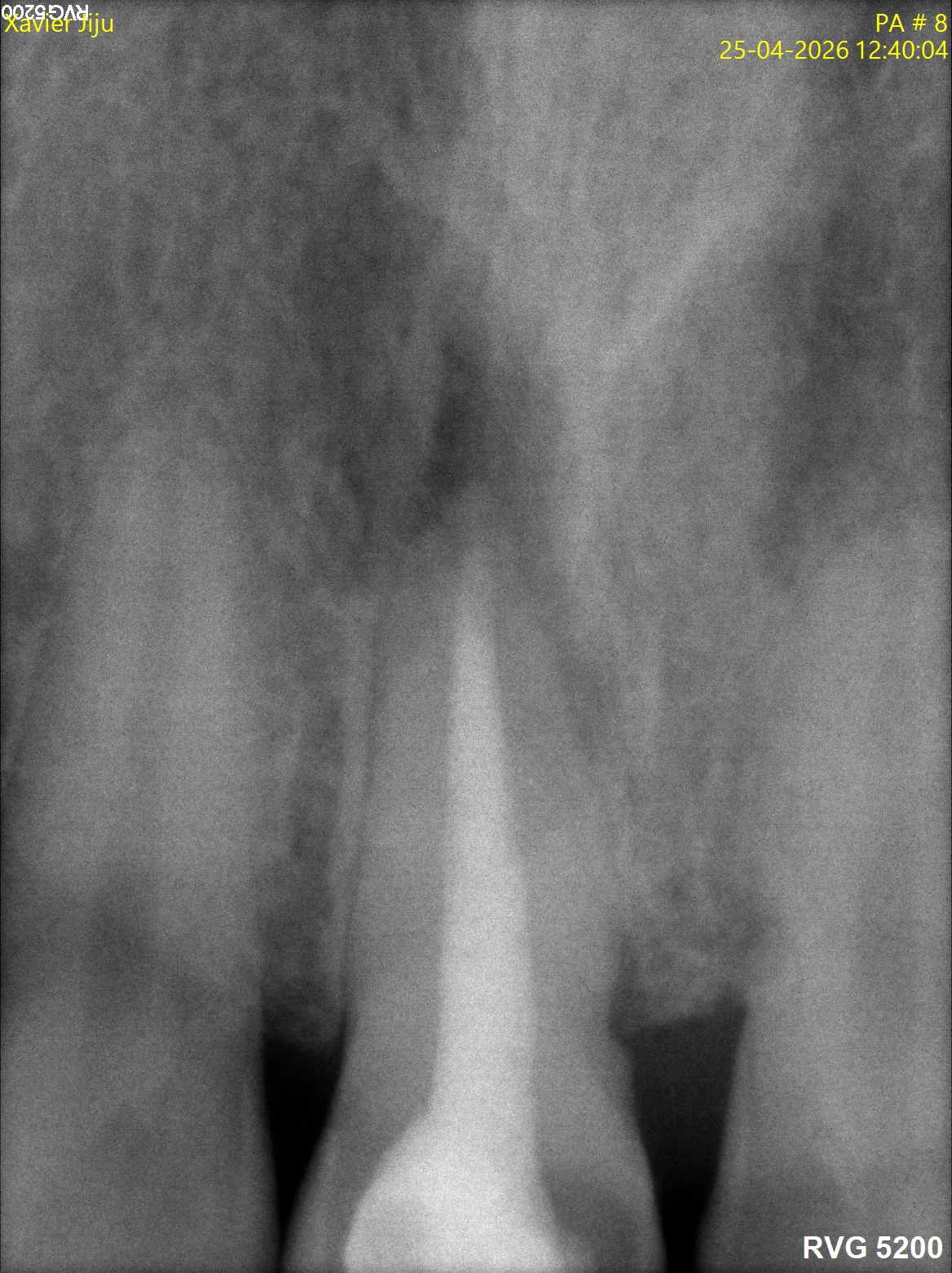
Infection Control with Root Canal

Upper front tooth needed management, decided to treat by Root Canal
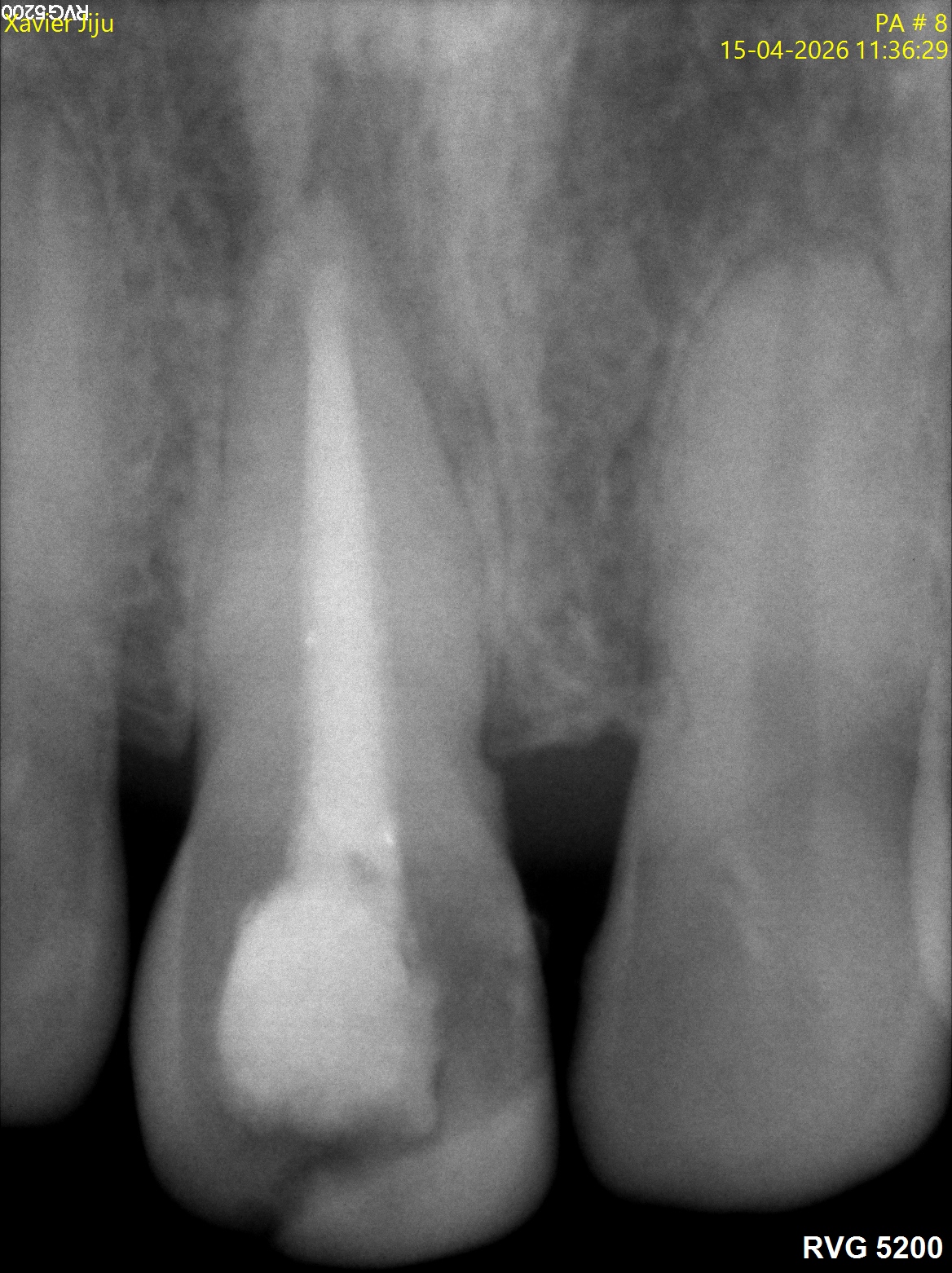
After Root canal treatment, along with MTA at the root end
Upper front tooth needed management, decided to treat by Root Canal
Re Root Canal

After root post placement and restoration

Tooth after Re root canal treatment.
Provides dental care to children from infancy to adolescence. Includes preventive care, fillings, and early orthodontic assessments. Trains in behavior management and child-friendly treatment. Educates parents on dental hygiene. Builds positive dental habits early in life.
Orthodontic Solutions
Modern alignment options for children, teens, and adults.
Spacing and Proclination

Before:

After:
Proclined Teeth

Before:

After:
Spacing and Proclination of Upper and Lower teeth

Before:

After:

Before:

After:
Spacing in Front Teeth and Rotation of a Tooth

Before:

After:
Overlapping Central Incisor

Before:

After:
Misaligned Teeth

Before:

After:
Crowding and Misaligned Teeth

Before:

After:
Diastemma and misaligned central incisors
Before:

After:
Focuses on gum and supporting bone health. Treats gum disease with cleaning, scaling, surgery, and maintenance. Plays a key role in preventing tooth loss. Supports implant procedures and gum aesthetics. Essential for long-term oral health.
Treatment plan
Periodontitis can be diagnosed by clinical examination using a periodontal probe and by radiographic examinination of bone loss. Periodontitis are painless and will be noted at a later stage only if individual is careless.
Preventive measures
Proper brushing twice a day, such a way that the bacterial plaque is disrupted and proper flossing daily.
Preserves natural teeth with minimal intervention. Treats cavities and damage with fillings, inlays, and sealants. Prioritizes early detection and treatment. Uses aesthetic materials for natural results. Helps avoid more invasive procedures.
Dental Composites
A new era in Dental restorative materials began in 1955 when Bunocre found that acrylic resin formed acceptable micro mechanical adhesion with dry dental canal that had been etched with phosphoric acid. Most Dental restorative resin systems are based on UDMA or BISGMA materials, with an added filler particles, which determines the final property of the composite which include the shade opacites, translucency and polish ability of the composites. When the flow of composite increases, the amount of filler particle is reduced, such composites have the disadvantage that the co-efficient of thermal expansion is more, leading to micro leakage and secondary caries, along restoration margins. Hybrid are a combination of micro fills and larger filter particles sizes the disadvantage is the inability to polish. Presently Nano hybrid Dental composites are the dental composites in the market, the choice of dental composites. Tooth coloured filling material should be decided by physical properties, amount of filler particles and size of filler particular, which decides the polish ability of the dental composite.
Advantages
It includes esthetics, which is one of the prime factor of composite restorations. Less tooth reduction when compared to amalgam restoration and it is insulative in nature and are added advantage is that it can be repaired when fracture of restoration occurs.
Disadvantages
The major disadvantage of composite is the shrinkage of composite, which is decided by two factors. The quality of Bond The shape of cavity The shape of the cavity effect in shrinkage of dental composite depends on the ratio of the bonded to unbounded surface of the preparation. The stress on the restoration increases, as the amount of bonded surface increases a class I restoration has five bonded and as unbonded surface. Taking into consideration of biocompatibility matter of dental composites, they cannot be placed in deep cavity directly, such deep cavities should be protected with a insulate barrier such as glass ionomer to protect pulp tissue. For a successful composite restoration, adequate time should be spent, curing each increment, provided a properly functioning light unit should be used and light guide should be as close as possible and at right angles to the material being photo curved.
Dental Amalgam
Dental amalgam is an alloy of silver tin, and small amounts of copper to which mercury is added. Depending on the amount of copper added it can be divided into high copper and low copper amalgam. High copper amalgam has better corrosion resistance than low copper amalgam. Depending an particle size Dental amalgam can be classified as i) Spherical or (ii) spheroid. Depending on Presence of copper (i) high copper are (ii) low copper Amalgam has its properties such as excellent compressive strength, but once the dental restoration of amalgam fractures due to occlusal load, correction of such a filling is difficult and the whole filling should be replaced. Dental composites or Dental amalgam has its our merits and disadvantages but at the end of the day the individual wants a filling which is stable and with out causing him any pain.
Replaces missing teeth with surgically placed implants. Implants support crowns, bridges, or dentures. Offers a durable and natural-feeling solution. Requires careful planning and bone evaluation. Restores chewing, speech, and confidence.




- Site of the implant
- Patient factors
- Implant factors
- Skill of the surgeon
Success for an implant
Patient factors Bone quality is important in the success of the implant. Bone quality can be divided into
Type1
Homogenous compact bone, throughout the entire jaw.
Type2
Core of dense trabecular bone; surrounded by compact bone of cortical plate.
Type3
Dense trabecular bone, with thin cortical bone.
Type4
low density trabecular bone with a thin cortical bone. (Type 1 ) and (type 2) ideal for implants.
Systematic Diseases: Diabetes -High uncontrolled diabetes can affect the blood supply of the bone thus chances of implant rejection is high.
Osteoporosis: Can affect the intergrity of the implant Irradiated Jaw,reduced blood supply, osteoradio necrosis xerostomia which are seen in radiation therapy can affect the implant. Ideally it is good to wait for 6-12 months before placing implant.
Infection: Infection at the site can be a reason for implant failure which should be looked into before implant is placed. Oral leshions can be a reason for implant failure.
Inproper oral hygiene: Plaque accumulation leads to inflammation and eventually leads to periodontitis and implant failure.
Age and sex: Has a role in implant failure since as we age the bone healing ability is reduced.
Oral Habbits: Smoking and bruxism can affect the intergrity of the dental implants. During bruxism, horizontal forceses are exerted on the dental implants, which can cause excessive osteoclastic activity at the site of implant and no osteo blastic activity at the region. So in an implant the forceses should be transmitted through the long axis of the implant. In bruxers by reducing the surface area of the crown, and also by increasing the length and width of dental implant effect of bruxism can be reduced.
The importance of site comes to play in bone quantity, quality and forceses of mastication the bone is subjected to, and close proximity to Endodontic restorations, which helps the Dentist to go far an implant, or avoid an implant. If going for an implant, the length and width of the implant choosen matters in bone selection. Bone augmentation or bone grafting which needs to be done in certain situations, can be a failure in the situations like osteoporosis periodontial disease or even infection which can affect the integrity of bone formation. Provided the timing of the placement of the implant in the grafted bone is important, time should be given for the grafted bone to mature and usually it takes 6-12 months for lamellar bone, which can adhere to implant interface. Bone grafting can be successful procedure, provided adequate blood supply to the area and micro movement of the implant doesn’t occur during the osteointegration stage.
Occlusal Forceses
Implants being ostio intergrated with bone doesnt have periodontal support as natural tooth, so shear forces are damaging to the implant. The implant and corresponding tooth should be designed in such a way that forces should be directed along the long axis of the implant, such a way that shear forceses are prevented from acting on the cervical margin of the tooth, especially on the buccal side of the implant. Forceses along the long axis of the implant are well tolerated, but shear forces not good, it can lead to bone loss on cervical area. Sites which are more posterior are subjected to more occlussal forces since they are close to the fulcrum of the mandible.
Implant Design (Factors)
Length of implant Average length of the implant used varies from 10-16mm, longer implant better bone contact which improves the stability of the implant to occlusal forces. Width of the implant Increase in width of the implant with grooves in the implant make the surface area contacted by the implant increases, which increases the stability of implant to occlusal forceses A healthy gingival sulcus of 3-4mm should maintained between the implant and crest of the alveolar bone. An implant placed next to a tooth should be at least 3 mm apart so as the provide adequate blood supply to the periodontal ligament. Implant to implant should be placed 4-7mm, to prevent bone necrotic and thus failure of implant.
Surgical Technique
When bone is exposed to temperature of (470C) for more than 1 minute, it results in collagen damage, bone necrosis and eventually death of bone, which results in collagen adhering to implant and bone, than proper osteo integration. This can happen when excessive pressure and excessive speed is applied during the drilling procedure of the implant, insufficient coolant is used during the drilling procedure far implant. Using a surgical length no. 2 round bur, the density and thickness of the bone can be evaluated.
Time of implant loading
Implant should be loaded depending on the density of the bone, from a period of four months to one year. Early loading can affect osteo- integration along the implant and finally the implant can end up in failure due to fibrous collagen formation between the implant and bone. Occlussion should be adjusted such a way that excessive forcesses should not be directed on the implant which can effect the ostiointegration of the implant. Provided the oral hygeine of the individual can affect the life of the implant, due to improper plaque removal and not using interdental cleansing aids, which can cause gum inflammation.
- Brush your teeth twice a day using fluoride toothpaste to remove plaque and bacteria.
- Clean between your teeth daily with dental floss or interdental brushes to prevent gum and tooth infections.
- Rinse your mouth after meals, especially if brushing isn’t possible.
- Limit sugary and acidic foods and drinks, as they encourage bacterial growth and tooth decay.
- Drink plenty of water, which helps wash away food particles and bacteria.
- Replace your toothbrush every 3–4 months or sooner if the bristles are worn.
- Avoid sharing toothbrushes or oral care items, as this can spread infections.
- Visit a dentist regularly for checkups and professional cleaning to detect problems early.
- Do not ignore pain, swelling, or bleeding gums—early treatment prevents serious infections.
- Avoid tobacco and limit alcohol, as they increase the risk of oral infections and gum disease.
Restorative Dentistry is the branch of dentistry concerned with diagnosing, preventing, and treating diseases of the teeth and supporting structures, and restoring damaged or missing teeth to normal function, health, and appearance.
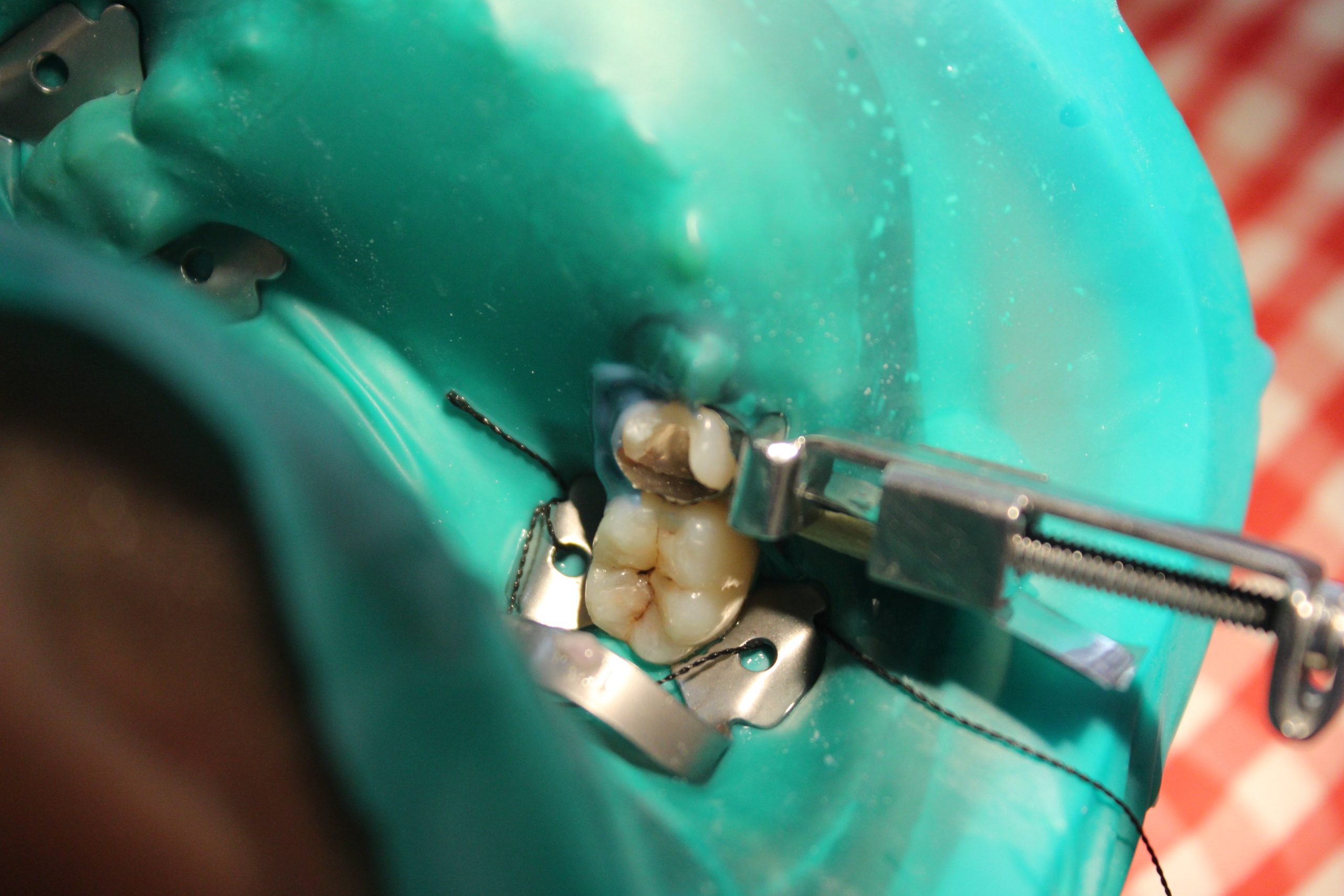
Needed filling of a decayed tooth , islated with rubber dam.

Decayed tooth filled with Tooth Coloured Filling material